01
Corneal Transplantation
Endothelial Keratoplasty — DSEK & DMEK
Layer-selective replacement of diseased endothelium while preserving anterior stroma and Bowman layer — the contemporary gold standard.



Thorough, unhurried consultations for corneal conditions, refractive concerns, and ocular surface disorders — scheduled at a time that suits you.
Modern ophthalmology is shifting from replacement toward restoration. Tissue preservation, minimally traumatic surgery, and biologically informed reconstruction produce more durable outcomes and more complete visual recovery.
Selective lamellar techniques spare healthy tissue — every decision begins with: what can we retain?
Surgery aligned with natural cellular architecture — from DMEK to limbal stem-cell procedures.
Individualised planning addressing higher-order aberrations and tear film-interface dynamics.
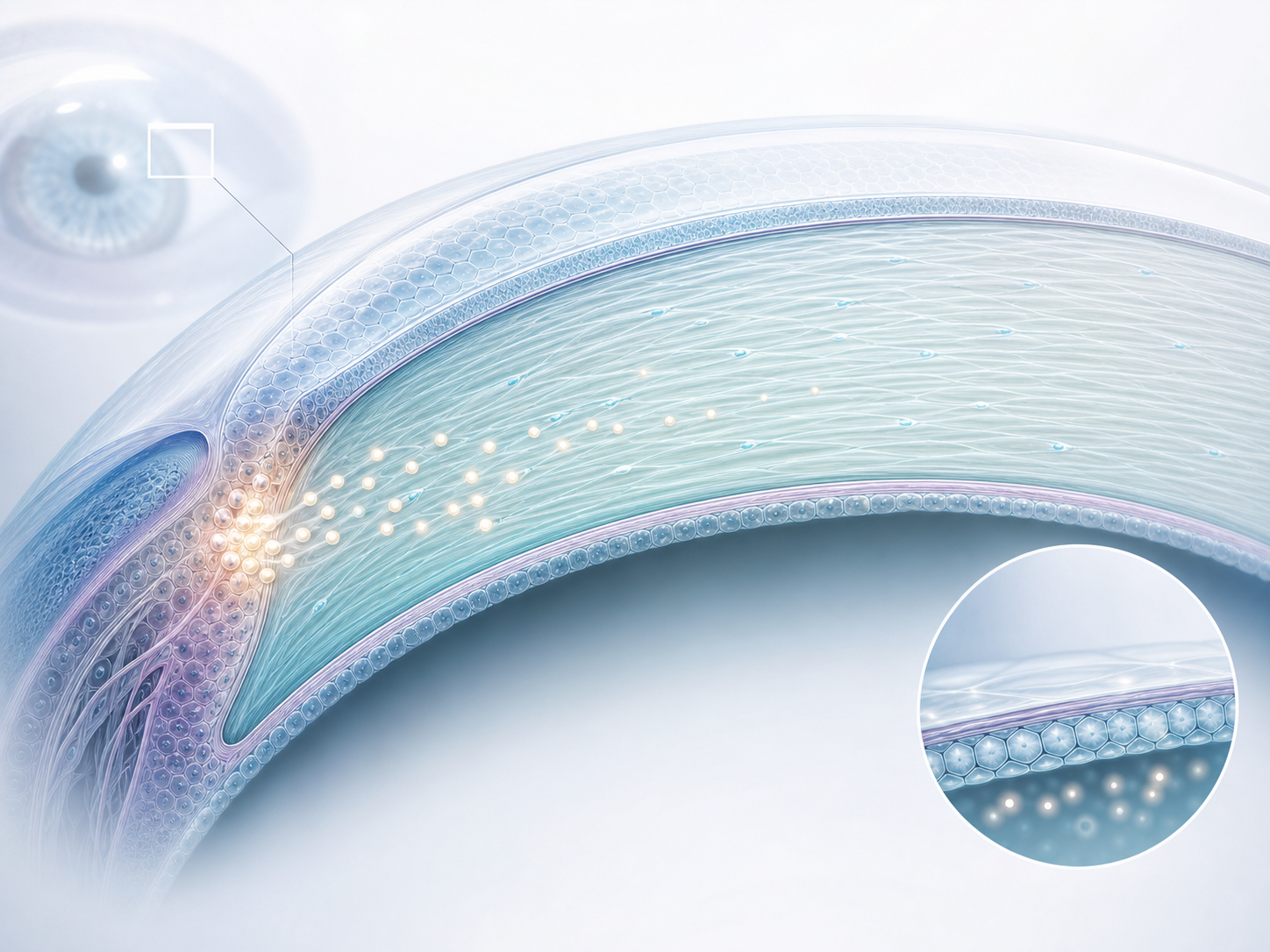
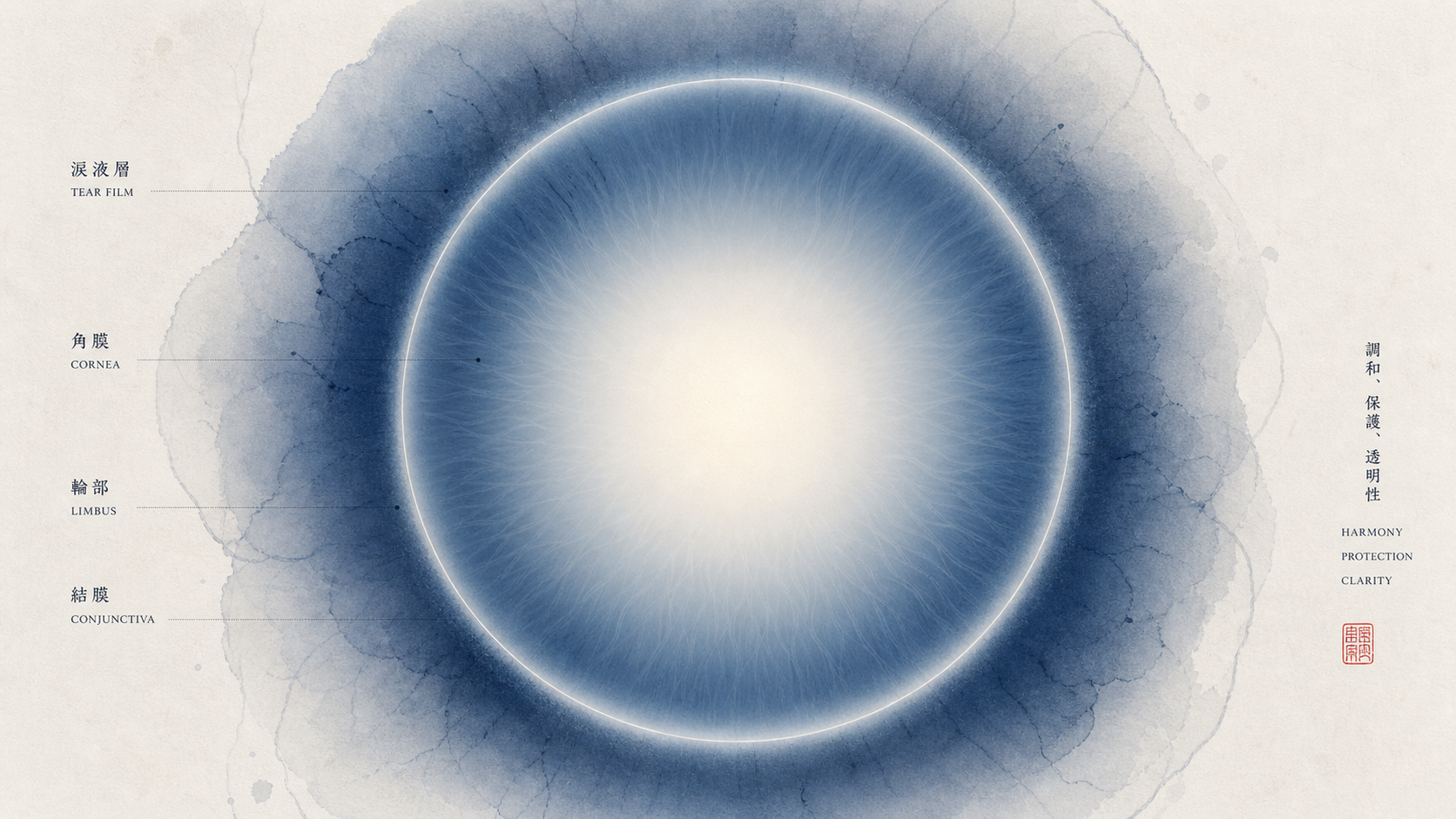
Corneal microanatomy — layers of biological function
Each service integrates surgical precision with a restorative mindset — preserving native tissue wherever biology permits.
Layer-selective replacement of diseased endothelium while preserving anterior stroma and Bowman layer — the contemporary gold standard.
Specialist reconstruction for limbal stem-cell deficiency from chemical injury, Stevens-Johnson syndrome, or chronic inflammation.

Bladefree flap creation, keratoplasty trephination, and SMILE lenticule extraction with micron-level precision.

Femtosecond-assisted phacoemulsification minimising endothelial stress, with precise capsulorhexis for optimal IOL centration.

Meibography-guided: cyclosporine A, IPL therapy, LipiFlow thermal pulsation, and autologous serum formulations.
Five principles that define every patient encounter — from first assessment to long-term optical rehabilitation.
We replace only the diseased layer — residual healthy anatomy is the most reliable scaffold for recovery.
Surface stability addressed before optimising refractive outcomes — visual quality and tear film are inseparable.
Every anterior segment procedure planned with corneal endothelial cell density in mind.
Ripasudil and netarsudil modulate CEC proliferation, offering adjunctive support in DSEK/DMEK recovery.
Graft survival, refractive stability, and surface homeostasis tracked longitudinally — decades in mind.
Not aspirational targets — the measurable standards that define our perioperative protocols, device selection, and pharmacological decisions.
Explore Cataract SurgeryMicroincision phacoemulsification reducing surgically induced astigmatism.
FLACS pre-fragmentation reduces phaco energy up to 43% vs manual technique.
Near-physiological endothelial replacement preserving all anterior layers.
Rho-kinase inhibitors modulating endothelial proliferation and wound healing.
An unstable ocular surface is the most common cause of visual dissatisfaction after successful surgery. We address the full spectrum of epithelial, glandular, and immunological contributors.
Chemical injury, Stevens-Johnson, aniridia — managed through CLAU, CLET, and cultivated procedures.
Managed with cenegermin (Oxervate) and specialised surface protection.
SJS, MMP — amniotic membrane transplantation and systemic immunosuppression.
Meibography-guided: IPL, LipiFlow, azithromycin, preservative-free lubricants.
Whether assessing a corneal condition, exploring refractive options, or managing a complex surface disorder — consultations are thorough, unhurried, and evidence-grounded.