Restorative
Ophthalmology
The eye does not simply tolerate surgery — it responds to it. Understanding how ocular tissues heal, and how modern clinical practice can support rather than override that biology, is the intellectual core of restorative ophthalmology.
What Restoration Really Means in Ophthalmology
Restoration in ophthalmology is not a single technology. It is a philosophy — one that asks how we can restore form, function, and optical quality by working with the eye's own healing biology.
The popular understanding of "biologic medicine" in eye care is often narrow. In ophthalmology, the truth is simultaneously more nuanced and more immediately applicable. Restoration encompasses every cellular and molecular process by which ocular tissues — the corneal epithelium, the stroma, the endothelium, the conjunctiva, the ocular surface glands, and the corneal nerve plexus — restore their architecture and function after disease or surgical trauma.
Modern restorative ophthalmology draws from wound healing biology, immunology, neuropathology, biomechanics, and pharmacology. Its clinical expression appears in decisions made before a patient enters the operating theatre — optimising the tear film, suppressing subclinical inflammation, preserving the limbal niche — and in choices made on the surgical table: the width of an incision, the energy delivered by a phacoemulsification handpiece, the choice of a tissue adhesive over a suture.
This article traces the science underlying each dimension of ocular healing, explains why these processes matter for visual outcomes, and describes how the principles of restorative ophthalmology are translated into clinical practice.
Biologic Healing
Harnessing the eye's intrinsic repair mechanisms — cytokine cascades, growth factors, resident immune cells — rather than overriding them with blunt interventions.
Tissue Preservation
Every layer of healthy tissue spared from unnecessary trauma represents preserved optical potential. Preservation is a therapeutic act in its own right.
Inflammation Control
Unregulated inflammation is the common pathway to fibrosis, haze, graft failure, and chronic surface disease — and the target of precise therapeutic intervention.
Precision Reconstruction
When tissue is lost beyond repair, replacing only the diseased layer — endothelium alone in DMEK, stroma selectively in DALK — rather than the entire cornea.
Visual Rehabilitation
Acuity is not the final goal. Contrast sensitivity, optical aberrations, neural adaptation, and quality-of-life metrics complete the picture of restored vision.
Ocular Surface First
No optical system — natural or artificial — performs optimally atop an unstable tear film or a compromised epithelial surface. Surface health precedes optical correction.
Corneal Immune Privilege — Why the Eye is Different
The cornea maintains tissue clarity in part by sustaining an active state of immune tolerance. This is not passivity — it is a precisely regulated biological achievement.
The concept of ocular immune privilege, first formally described by Sir Peter Medawar in the 1940s, refers to the eye's capacity to tolerate foreign antigens without mounting the destructive inflammatory responses seen in other tissues. This privilege is not merely the result of physical barriers — it is an active, multi-layered system maintained by soluble immunosuppressive factors, specialised cell populations, and anatomical arrangements that limit antigen presentation.
The avascular corneal stroma is central to this privilege. The absence of blood and lymphatic vessels in the central corneal stroma limits the afferent arc of immune surveillance, meaning that foreign antigens encounter fewer antigen-presenting cells and are less efficiently transported to regional lymph nodes. This avascularity is not incidental to corneal function — it is inseparable from corneal transparency.
Corneal immune privilege is sustained by several mechanisms acting in concert. Transforming growth factor-beta (TGF-β) in the aqueous humour actively suppresses T-cell activation. Fas ligand (FasL) expression on corneal cells induces apoptosis in infiltrating inflammatory cells. Complement regulatory proteins on corneal endothelium limit lytic membrane attack. Regulatory T cells (Tregs) in both the anterior chamber and the corneal tissue itself participate in maintaining tolerance.
In clinical practice, this privilege is fragile. Corneal neovascularisation — the ingrowth of new blood vessels into the normally avascular stroma — directly undermines immune privilege and dramatically increases the risk of allograft rejection after corneal transplantation. Managing neovascularisation before and after surgery is therefore immunological risk reduction, not cosmetic management.
"Corneal immune privilege is an active biological achievement, not a passive anatomical accident. Preserving it is as important as preserving the tissue itself."
The Biology of Transparency
Corneal transparency is one of the most extraordinary properties in vertebrate biology — and one of the most metabolically demanding to maintain.
The cornea transmits approximately 90% of incident visible light. This transparency depends on the precise arrangement of collagen fibrils within the stroma — uniformly small diameter (25–35 nm), regularly spaced (roughly 65 nm centre-to-centre), and organised in orthogonally arranged lamellae. This lattice arrangement causes destructive interference of scattered light, allowing net light transmission to approach theoretical maxima.
This arrangement is maintained by keratocytes — the resident stromal fibroblasts — and by the continuous deturgescing action of the corneal endothelium. Corneal transparency depends critically on relative dehydration: the stroma must remain at approximately 78% water content. The endothelium achieves this through a coupled sodium-bicarbonate transport system, pumping fluid out of the stroma against an osmotic gradient. Loss of even 30% of endothelial cell density begins to compromise this function.
The crystalline proteins within keratocytes also contribute to transparency at the cellular level, reducing light scatter from cell bodies in a manner analogous to the lens crystallins — a convergent evolutionary strategy across different transparent ocular tissues.
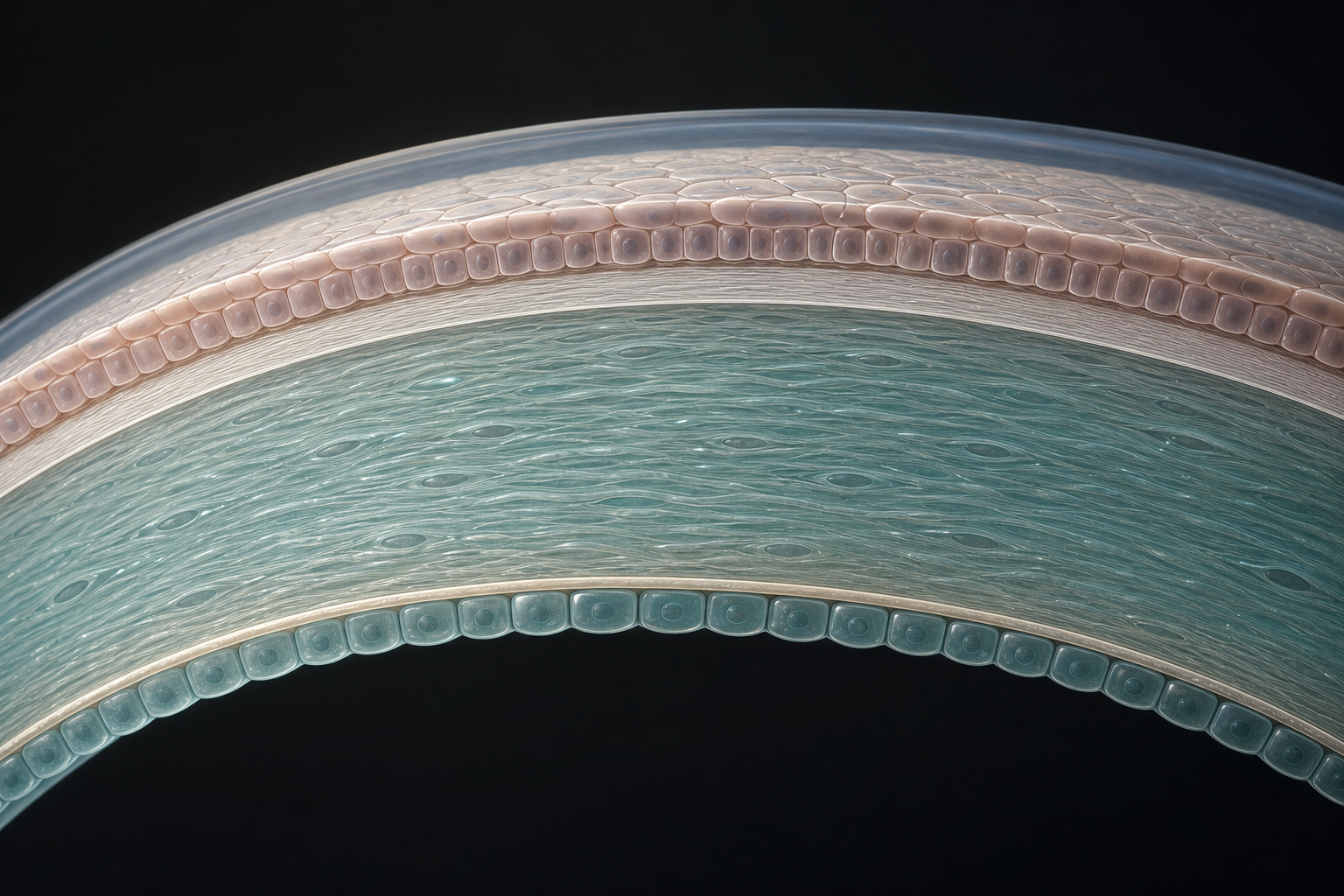
Figure 1. The five structural layers of the human cornea — epithelium (50 µm), Bowman's layer (8–14 µm), stroma (~500 µm, 90% of thickness), Descemet's membrane (10–12 µm), and endothelium (~2,000–3,500 cells/mm²).
Epithelial Healing & The Ocular Surface
The corneal epithelium is the most regeneratively capable layer of the eye — provided its stem-cell niche remains intact.
The corneal epithelium is a stratified, non-keratinised squamous epithelium five to seven cell layers deep. It turns over completely approximately every seven to ten days under normal conditions, driven by a unidirectional centripetal migration of daughter cells from the limbal stem-cell niche at the corneoscleral junction. This population of limbal epithelial stem cells (LESCs), residing in specialised anatomical invaginations termed the Palisades of Vogt, is the restorative foundation of the ocular surface.
When a corneal abrasion occurs, the response is rapid and tightly co-ordinated. Within hours, the wound edges flatten and lamellipodia extend over the denuded basement membrane, driven by integrin-mediated adhesion signals, EGF receptor activation, and hepatocyte growth factor (HGF) released from the stroma. The epithelium does not simply divide and fill — it migrates as a coherent sheet, a process termed collective cell migration, preserving tight-junction integrity and barrier function as it advances.
Limbal stem-cell deficiency (LSCD) — whether from chemical injury, Stevens-Johnson syndrome, aniridia, chronic contact-lens hypoxia, or repeated surgeries — disrupts this system entirely. Without a functioning limbal niche, conjunctival epithelium migrates centrally onto the cornea (conjunctivalisation), bringing with it goblet cells, inflammatory mediators, and the risk of neovascularisation.
Treatment of LSCD requires restoration of the limbal niche — through cultivated limbal epithelial transplantation (CLET), conjunctival-limbal autograft (CLAU), or living-related allograft (lr-CLAL) — before any further optical rehabilitation is attempted. This principle — surface before optics — is axiomatic in restorative ophthalmology.
The corneal stroma is populated by keratocytes — quiescent, transparent, dendritic cells that maintain the extracellular matrix between surgical or disease episodes. Upon injury, keratocytes surrounding the wound undergo apoptosis (a process mediated by Fas–FasL signalling from damaged epithelial cells). The surviving keratocytes adjacent to the wound zone then activate, transforming into fibroblasts and subsequently myofibroblasts under the influence of TGF-β₁ released from the epithelium.
Myofibroblasts are the central cellular mediators of corneal fibrosis. Unlike quiescent keratocytes, myofibroblasts express α-smooth muscle actin, have disordered cytoskeletal architecture, produce irregular extracellular matrix components (including type III collagen, fibronectin, and tenascin-C), and lack the crystallin proteins that contribute to cellular transparency. They scatter light. A wound populated by myofibroblasts is a wound in fibrotic remodelling — and the clinical correlate is corneal haze or stromal opacity.
Whether a wound resolves with clarity or persists with opacity depends on the persistence of TGF-β₁ signalling and the integrity of the epithelial barrier above. An intact epithelial basement membrane limits TGF-β penetration into the stroma; disruption of that membrane — as occurs in photorefractive keratectomy, severe epithelial disease, or recurrent erosions — permits sustained myofibroblast activation and haze formation.
This is why management of stromal wound healing focuses on supporting epithelial recovery and limiting TGF-β signalling — through topical steroids, antimetabolites (mitomycin-C in appropriate contexts), and targeted therapies aimed at TGF-β receptor pathways.
Stromal Remodelling & How Fibrosis Obscures Vision
Fibrosis is the shadow side of healing — the mechanism that closes wounds but, in doing so, disrupts the precise architecture on which transparency depends.
Corneal Nerve Repair
The cornea is the most densely innervated tissue in the human body — and one of the most frequently damaged by surgery and disease.
The human cornea contains approximately 7,000 nociceptive nerve endings per square centimetre, derived from the ophthalmic division of the trigeminal nerve. These fibres travel as a dense sub-basal nerve plexus just beneath the corneal epithelium, where they are identifiable by in vivo confocal microscopy as a network of bright, branching fibres of extraordinary delicacy.
Corneal nerves are not merely sensory — they are trophic. They release substance P, calcitonin gene-related peptide (CGRP), and neuropeptide Y, which sustain epithelial mitotic activity, tight-junction integrity, and normal tear production. Denervation — whether from LASIK flap creation, herpes simplex keratitis, diabetes mellitus, or trigeminal neuralgia — reduces this trophic support and produces neurotrophic keratopathy (NK).
SMILE (small incision lenticule extraction) causes significantly less nerve damage than LASIK due to the absence of a stromal flap — now a recognised clinical advantage of small-incision refractive approaches. Cenegermin (recombinant human nerve growth factor, rhNGF) — approved for neurotrophic keratopathy — directly supplements the trophic signalling lost to corneal denervation, promoting epithelial healing without surgical intervention.

Endothelial Homeostasis & Recovery
The corneal endothelium is the eye's most critically non-self-renewing tissue — and the primary target of modern lamellar transplantation.
The corneal endothelium is a monolayer of hexagonal cells lining the posterior corneal surface. Normal density in young adults is approximately 3,000–3,500 cells/mm²; this declines naturally at 0.3–0.6% per year with age. Unlike most other tissues, the corneal endothelium has severely limited capacity for self-renewal in vivo: cell division is actively suppressed by TGF-β₂ in the aqueous humour, which maintains the cells in G₁ phase arrest. Cell loss is compensated by spreading and enlargement of surviving cells, not by division.
This limited capacity makes endothelial cell density a non-renewable resource. Every surgical intervention reduces it to some degree. Cumulative endothelial cell loss from cataract surgery with conventional phacoemulsification ranges from 8% to 18% — which is why cumulative dissipated energy (CDE) reduction directly translates into preserved endothelial function.
Rho-associated kinase (ROCK) inhibitors such as ripasudil and netarsudil have demonstrated the capacity to stimulate endothelial cell migration and limited proliferation in laboratory and early clinical settings, offering the prospect of non-surgical endothelial recovery in carefully selected patients.
Healthy Endothelial Reserve
Regular hexagonal cell morphology; uniform cell size; near-perfect pump function maintaining stromal hydration at ~78%.
Compensatory Phase
Polymegethism and pleomorphism increase; cells enlarge to cover loss. Cornea remains clear but surgical and disease risk is elevated.
Decompensation Risk
Any additional surgical trauma or disease episode may precipitate corneal oedema. Intraoperative energy minimisation is critical.
Decompensation — Surgery Required
Persistent stromal oedema; bullous keratopathy; painful epithelial breakdown. DSEK or DMEK is indicated.
The Tear Film as a Healing Substrate
The tear film is the first optical surface the eye presents to the world — and the first barrier between healing tissue and the environment.
"Ocular surface disease is a surgical risk factor, not merely a symptomatic condition."
The tear film is a complex, multi-component fluid comprising an outer lipid layer (secreted primarily by the Meibomian glands), an aqueous-mucin phase (secreted by the lacrimal gland and goblet cells of the conjunctival epithelium), and a glycocalyx-anchored mucin layer at the epithelial surface. Its roles are multiple: optical (providing a smooth refractive surface), mechanical (lubricating the eyelid-globe interface), and trophic (delivering growth factors, antimicrobial proteins, and oxygen to the avascular corneal epithelium).
Dry eye disease (DED), as defined by TFOS DEWS II, is a multifactorial disease of the ocular surface characterised by loss of homeostasis of the tear film. It is not merely an uncomfortable condition — it is a pathophysiological state that sustains chronic epithelial inflammation, impairs epithelial healing after surgery or disease, and reduces the optical quality of the eye's first refractive surface, elevating higher-order aberrations measurably even when the cornea appears clinically intact.
Autologous serum eye drops — prepared from the patient's own peripheral blood — contain EGF, TGF-β, fibronectin, and vitamin A at concentrations approximating natural tears, and represent a biologically rational approach to tear film support in severe ocular surface disease where conventional drops are insufficient.

Graft Integration & Corneal Transplantation
The modern era of corneal transplantation is defined not by tissue replacement, but by tissue precision — replacing only what is irreparably damaged and preserving everything that can be saved.
Full-thickness penetrating keratoplasty (PKP) — the dominant corneal transplant technique of the twentieth century — replaces the entire cornea and is associated with high astigmatism, suture-related complications, long recovery times, and a lifetime risk of rejection. The twenty-first century has been defined by the systematic decomposition of PKP into layer-specific surgeries.
Graft integration depends on the endothelial cells of the donor tissue adhering to the recipient's posterior corneal surface, establishing a functional pump mechanism, and gradually achieving sufficient density to maintain corneal deturgesence. Each generation of lamellar surgery has narrowed the tissue transplanted, improving outcomes and reducing rejection risk.
PKP
Replaces the entire cornea. Associated with high astigmatism, suture complications, and lifelong rejection risk from multiple tissue antigens. Now reserved for cases where lamellar surgery is not feasible.
DALK
Replaces epithelium, Bowman's, and stroma while preserving the patient's own Descemet's membrane and endothelium — eliminating endothelial rejection risk entirely. Procedure of choice in keratoconus and anterior stromal dystrophies.
DMEK
Transplants Descemet's membrane and endothelium alone (~15 µm). Achieves superior visual acuity with lower rejection rates. Now the standard of care for Fuchs' dystrophy in experienced centres. 5-year survival 80–90%.
The eye measures light with extraordinary precision. A healthy cornea contributes approximately 43 dioptres of refracting power; both cornea and crystalline lens depend on smooth, regular, precisely curved surfaces to deliver coherent wavefronts to the retina. Any disruption of surface regularity — epithelial irregularity, stromal haze, graft interface oedema, tear film instability — degrades the quality of the wavefront before it reaches the photoreceptors, reducing contrast sensitivity and increasing higher-order aberrations even when Snellen acuity measures 6/6 or better.
This is the clinical meaning of the phrase "healing quality determines visual quality." A cornea that heals with irregular epithelium, sub-epithelial fibrosis, or persistent inflammation produces a degraded optical surface regardless of the technical precision of the surgery that preceded it. Conversely, a cornea that heals with smooth epithelium, transparent stroma, and a stable tear film is an excellent refractive substrate.
In practical terms, this means that the perioperative period — before, during, and after surgery — is as important as the surgery itself. Pre-operative optimisation of the ocular surface, anti-inflammatory prophylaxis during the healing phase, nerve-supportive topical therapy, and tear film supplementation are not adjuncts to good surgery: they are components of it.
Why Healing Quality Determines Visual Quality
Vision is an optical phenomenon — but optical quality is ultimately a biological one.
"Visual acuity measures one dimension of what a patient sees. Healing quality determines the rest: contrast, depth, colour fidelity, and comfort in light."
Principles of Minimally Traumatic Surgery
The surgeon's goal is not only to achieve the intended anatomical result — it is to achieve that result with the minimum biological cost to the tissues that must then heal.
Minimally traumatic surgery is a philosophy applied consistently across all decisions in the operating theatre. At the incision level, it means the smallest wound compatible with the required surgical access: 2.2 mm or smaller for modern phacoemulsification, 2.75 mm or smaller for DMEK roll delivery, sutureless where achievable. At the energy level, it means minimising phacoemulsification ultrasound energy — measured as cumulative dissipated energy (CDE) — which is directly correlated with corneal endothelial cell loss and anterior chamber inflammation.
At the pharmacological level, it means preferring preservative-free formulations wherever available, recognising that benzalkonium chloride (BAK) is cytotoxic to corneal epithelial cells at clinical concentrations, inhibits conjunctival goblet cells, and sustains ocular surface inflammation.
Intraoperative viscoelastic selection is part of the same calculus: cohesive viscoelastics protect the endothelium during phacoemulsification but are associated with higher post-operative intraocular pressure spikes; dispersive viscoelastics coat the endothelium better but are harder to aspirate. Combination ("soft-shell") techniques optimise for both. This is the level of granularity at which minimally traumatic surgery operates.
Myth vs. Fact
Common misconceptions about restorative ophthalmology, corrected.
"Biologic eye care means stem-cell eye drops that restore vision."
This framing conflates speculative consumer products with the evidence-based clinical science of tissue repair, immune regulation, and biologically intelligent surgery.
Restoration encompasses epithelial repair, nerve recovery, endothelial homeostasis, and graft integration — most of which occur without any cell transplantation.
CLET and CLAU are evidence-based LESC restoration procedures; other "stem-cell" eye products lack peer-reviewed clinical validation.
"If my vision is 6/6 after surgery, the eye has healed perfectly."
Snellen acuity is a single, coarse metric. Many eyes with 6/6 acuity have significantly compromised contrast sensitivity, elevated higher-order aberrations, or chronic surface inflammation.
Visual quality encompasses contrast sensitivity, mesopic function, wavefront aberrations, and tear film stability — all of which depend on tissue healing quality.
Patient-reported outcomes often diverge from acuity measurements, precisely because acuity does not capture the full optical impact of incomplete healing.
"The cornea cannot heal — damage is permanent."
This conflates the limited capacity of the endothelium (true) with the remarkable capacity of the epithelium and the partial capacity of the stroma (both false).
The corneal epithelium renews completely every 7–10 days; stromal wounds remodel over months; endothelial recovery is limited but pharmacologically augmentable with ROCK inhibitors.
Healing capacity is layer-specific. Treatment must be tailored accordingly.
"Dry eye is just discomfort — it doesn't affect surgical outcomes."
This underestimates the systemic impact of ocular surface disease on biometry accuracy, wound healing, visual recovery, and patient satisfaction.
Pre-operative DED causes corneal topography irregularity that can produce 0.5–1.0 D IOL prediction errors in cataract surgery.
Ocular surface disease is a surgical risk factor, not merely a symptomatic condition.
"Corneal transplantation is high-risk and rarely successful."
This reflects the historical framing of full-thickness PKP, which has now been substantially superseded by layer-specific lamellar approaches.
DMEK has a 5-year graft survival of approximately 80–90% in Fuchs' dystrophy; DALK eliminates endothelial rejection risk entirely.
Modern lamellar corneal transplantation represents one of the most successful tissue transplant procedures in medicine.
Frequently Asked Questions
Evidence-based answers to the questions most commonly asked by patients and families.
It means that your treatment plan is designed not merely to correct a refractive error or remove a cataract, but to consider how your eye heals before, during, and after intervention. This includes optimising your tear film and ocular surface before surgery, choosing techniques that minimise tissue trauma, selecting medications that support your eye's healing biology, and monitoring recovery with the same attention given to the procedure itself. It is a continuity of care, not a single event.
Dry eye causes tear film instability and surface irregularity that affects the accuracy of pre-operative measurements (biometry) used to calculate your intraocular lens power. Studies have demonstrated that untreated DED can cause IOL power prediction errors of up to 1 dioptre. Treating the surface before surgery produces more accurate biometry, better refractive outcomes, and faster visual recovery.
LASIK creates a corneal flap that severs the stromal nerve bundles as they enter from the limbus. The sub-basal nerve plexus in the central cornea is significantly reduced immediately post-operatively. Partial recovery occurs by 3–6 months, but full return to pre-operative density may take 12–24 months, and some studies suggest incomplete recovery even at 5 years. SMILE causes substantially less nerve disruption because it avoids flap creation.
Limbal stem-cell transplantation has been a validated, peer-reviewed clinical procedure for over three decades. CLAU, lr-CLAL, and CLET are all supported by clinical evidence. Holoclar (EMA-approved) is the first approved cell therapy product for LSCD in Europe. These are evidence-based surgical procedures within mainstream corneal practice.
Both are forms of endothelial keratoplasty. DSEK transplants a thin disc of posterior stroma along with the membrane and endothelium — typically 100–150 µm thick. DMEK transplants only the membrane and endothelium (~15 µm), without any stroma. DMEK typically achieves better visual acuity and lower rejection rates due to the absence of a stromal interface, but it is technically more demanding. The choice depends on your anatomy, the surgeon's experience, and your individual disease.
In normal circumstances, corneal endothelial cells do not divide in the adult eye. However, ROCK inhibitors such as ripasudil and netarsudil have demonstrated the ability to promote endothelial cell migration and limited proliferation in laboratory and early clinical settings. Descemetorhexis without endothelial keratoplasty (DWEK) has shown promise in select patients with Fuchs' dystrophy. These remain areas of active investigation.
Neurotrophic keratopathy (NK) is a degenerative condition caused by damage to the trigeminal nerve supply of the cornea — from herpetic keratitis, diabetes, corneal surgery, or trigeminal nerve injury. The reduction in trophic neuropeptides impairs epithelial healing, resulting in persistent epithelial defects, stromal ulceration, and risk of perforation. Cenegermin (Oxervate), a recombinant human nerve growth factor, directly supplements the lost trophic signal, producing corneal healing rates significantly superior to vehicle in controlled trials.
Scientific References & Landmark Concepts
The clinical content of this article is grounded in the following peer-reviewed literature and foundational ophthalmology research.
Healing is not passive.
It can be guided.
If you have questions about your corneal health, ocular surface condition, or surgical options, our clinical team combines surgical expertise with the full depth of restorative ophthalmology.