The cornea and ocular surface form a living biological interface composed of epithelium, limbal stem-cell niches, tear film, corneal nerves, eyelids, meibomian glands, conjunctiva, and immune mediators. When this ecosystem becomes chronically inflamed or structurally unstable, healing slows, epithelial failure becomes more likely, and clarity can be lost through ulceration, fibrosis, and scarring.
Modern cornea care therefore focuses on restoration as well as repair: stabilizing the surface environment, supporting epithelial regeneration, protecting corneal innervation, and selecting reconstructive procedures that preserve biology while rebuilding function.
How the ocular surface heals
The corneal epithelium is a self-renewing barrier whose repair depends on epithelial migration, proliferation, differentiation, extracellular matrix remodelling, and coordinated signalling between growth factors, keratocytes, inflammatory mediators, and corneal nerves. Tear film stability is part of this healing system, not merely a comfort layer.

Epithelial regeneration
Normal corneal epithelial healing usually proceeds over roughly 7 to 14 days after injury, provided the basement membrane and stromal microenvironment can support reattachment and orderly resurfacing. When the limbal stem-cell reserve is depleted, the basement membrane is abnormal, or stromal injury is deeper, healing becomes delayed and the risk of persistent epithelial defects, stromal melt, infection, and scarring rises substantially.
Why chronic inflammation impairs healing
Inflammatory cytokines such as TNF-alpha and IL-1 participate in normal wound signalling, but excess or persistent inflammation drives matrix degradation, stromal remodelling, epithelial instability, and in severe cases stromal melting. Ocular surface disorders such as dry eye disease, mucous membrane pemphigoid, Stevens-Johnson syndrome, and infectious keratitis can convert a reparative response into a destructive one.
Why lubrication is biologically important
Lubrication is not a cosmetic add-on to ocular surface care. The tear film contributes to corneal transparency and smoothness, and tear retention helps preserve access to growth factors and a more favourable environment for epithelial migration and adhesion. Preservative-free lubrication is therefore a biological support strategy, especially in persistent epithelial defects and neurotrophic disease.
The ocular surface is an ecosystem.
Corneal nerves, epithelial cells, meibomian glands, conjunctival goblet cells, and the lacrimal functional unit work together to sustain surface clarity and comfort. Nerve injury or severe surface disease can reduce blink quality, tear secretion, and trophic support, creating a cycle of epithelial breakdown and worsening inflammation.
Neurotrophic keratopathy is a reminder that the cornea is not only optical tissue, but also neurobiological tissue. Expert consensus emphasises that reduced corneal sensitivity, persistent epithelial defects, prior herpetic disease, diabetes, and trigeminal nerve injury should increase clinical suspicion because early recognition offers the best opportunity to prevent ulceration, stromal thinning, and vision loss.
From tear-film dysfunction to ocular surface failure
Corneal and ocular surface disease exists on a spectrum. Some disorders begin with tear-film instability and epithelial stress, while others involve limbal failure, sensory denervation, cicatricial change, active infection, or established fibrosis.
Dry eye disease
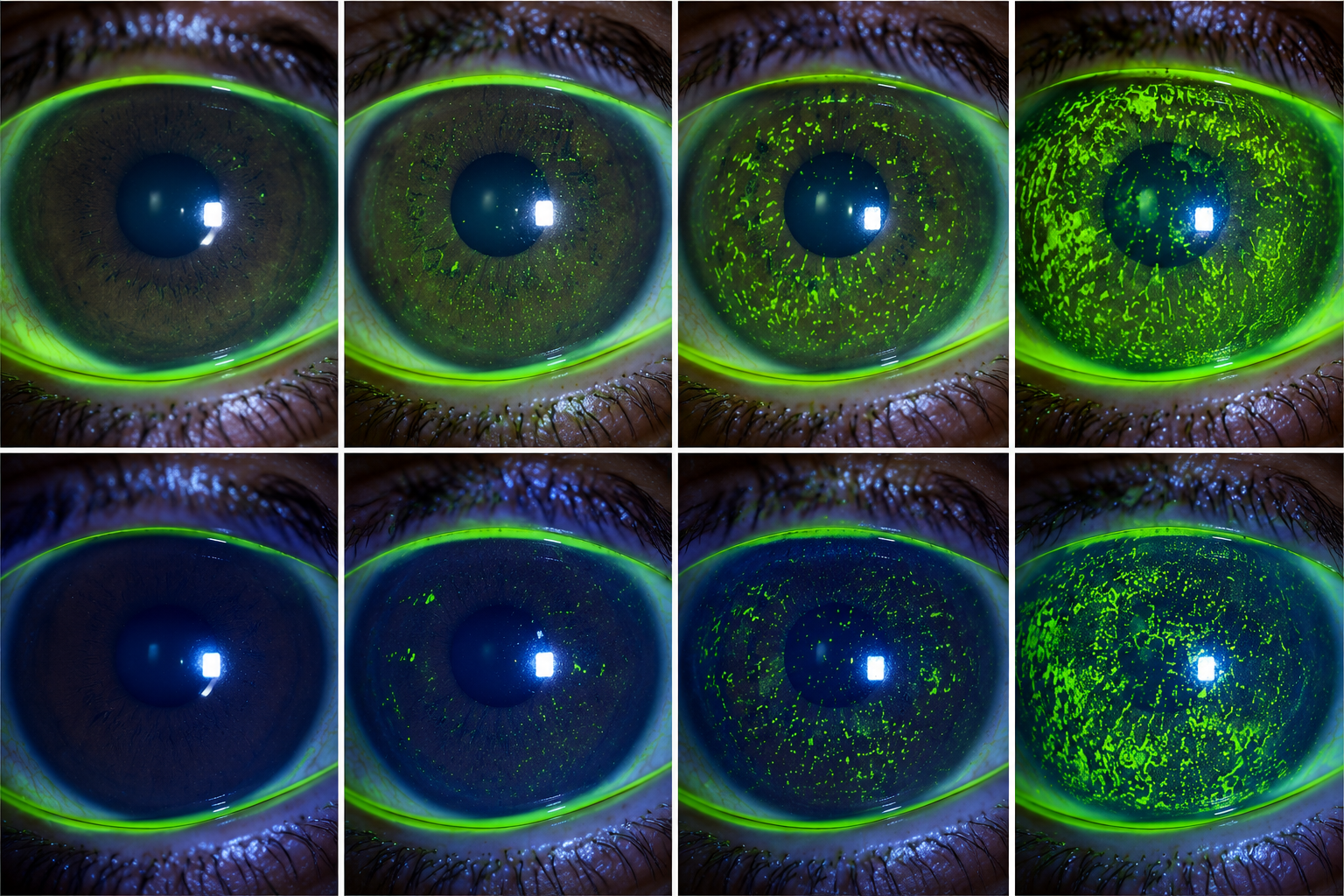
Dry eye disease is often a disorder of tear-film instability, inflammation, neurosensory dysfunction, and meibomian gland compromise rather than simple aqueous deficiency alone. Chronic tear dysfunction destabilises the epithelium, increases staining, amplifies inflammatory signalling, and can undermine surgical as well as medical outcomes.
Limbal stem-cell deficiency
Limbal stem-cell deficiency impairs the eye's capacity to regenerate healthy corneal epithelium and may lead to conjunctivalization, vascularisation, persistent epithelial defects, stromal scarring, and severe visual loss. Chemical injury, ocular surface burns, and autoimmune cicatrising disease are recognised causes.
Neurotrophic keratitis
Neurotrophic keratitis is a degenerative corneal disease caused by damage to trigeminal innervation, with progression from epithelial change to persistent defects, ulceration, stromal melting, perforation, and vision loss if untreated. Because symptoms may be surprisingly mild, corneal sensitivity testing and careful staging are essential.
Severe ocular surface disease
Severe ocular surface disease includes complex states in which lubrication, epithelial renewal, eyelid function, immune control, and stromal protection all become difficult simultaneously. Examples include Stevens-Johnson spectrum disease, graft-versus-host disease, severe chemical injury, and chronic exposure-related breakdown.
Corneal ulcers
Corneal ulcers represent stromal involvement and require urgent evaluation because infection, melt, perforation, and visually significant fibrosis can follow rapidly. The therapeutic goal is not only antimicrobial or anti-inflammatory control, but preservation of tissue architecture and prevention of further surface collapse.
Corneal scars
Corneal scars develop when healing becomes fibrotic rather than transparent. Once the extracellular matrix is reorganised irregularly and myofibroblast activity predominates, light scatter increases and visual quality may remain impaired even after the original injury has resolved.
Reconstructive care is layered, not singular.
The most effective ocular surface programmes combine biological support, anti-inflammatory control, mechanical protection, and reconstructive surgery when required. The treatment pathway depends on why healing has failed, not simply on what the cornea looks like in one photograph.

Serum tears and blood-derived biological support
Autologous serum contains vitamin A, epidermal growth factor, transforming growth factor-beta, platelet-derived growth factor, insulin-like growth factor, nerve growth factor, fibronectin, and other components relevant to epithelial recovery. Reviews of persistent epithelial defects describe serum tears as a biologically meaningful option for re-epithelialization, particularly in severe ocular surface disease and neurotrophic states.
Amniotic membrane transplantation
Amniotic membrane provides a scaffold for epithelial migration and has anti-inflammatory, anti-scarring, and anti-vascular effects that make it valuable in persistent epithelial defects, non-healing ulcers, and surface reconstruction. Consensus recommendations consider self-retained or transplanted amniotic membrane an appropriate or optimal component of care in moderate to severe disease.
Mucous membrane grafting
Mucous membrane grafting is used when cicatricial disease, lid margin keratinisation, or conjunctival deficiency creates chronic surface trauma and prevents epithelial stability. Its role is to re-establish a more physiologic mucosal interface and reduce recurrent mechanical injury.
Minor salivary gland transplantation
Minor salivary gland transplantation is a specialised reconstructive option for severe dry eye disease when conventional tear support is insufficient. Recent meta-analytic data reported symptomatic improvement in approximately 73.6% of patients, with mean improvements in Schirmer testing, tear break-up time, and corneal staining.
Ocular surface reconstruction
Ocular surface reconstruction may involve staged optimisation of inflammation, lubrication, epithelial support, corneal protection with bandage or scleral devices, amniotic membrane use, limbal restoration strategies, and adjunctive reconstructive procedures. The objective is to restore a surface capable of remaining closed, smooth, and biologically self-sustaining.
Restorative ophthalmology does not mean promising biological miracles. It means using credible, evidence-informed strategies that improve the conditions required for epithelial renewal, stromal protection, nerve-supported healing, and long-term surface stability.
What patients should understand about healing and scarring
Patients often expect the cornea to heal like skin. In reality, the ocular surface must heal while remaining smooth, transparent, and precisely organised at a microscopic level.
Why some eyes do not heal on time
Delayed healing can occur when the tear film is unstable, the limbal stem-cell reserve is reduced, the cornea has lost sensation, inflammation is excessive, infection is active, or the lids continue to traumatise the surface. In these situations, even a small epithelial defect may behave like a complex biological wound.
Why fibrosis affects vision
When the cornea heals with fibrosis, the newly repaired tissue is stronger than an open wound but not optically identical to native transparent cornea. Light scatter, irregularity, vascularisation, and haze may reduce quality of vision even when the eye is no longer painful or inflamed.
Why ongoing lubrication still matters after surgery or healing
Even after the surface appears closed, lubrication and surface support often remain essential because the cornea may still be rebuilding epithelial adhesion, neural feedback, and tear-film stability. Recovery of function can therefore continue beyond visible closure of the defect.
Common questions about corneal surface restoration
These answers are designed for an informed patient audience while remaining aligned with contemporary cornea practice.
No. Dry eye disease often involves inflammation, tear-film instability, meibomian dysfunction, epithelial stress, and neurosensory abnormalities rather than reduced tears alone.
It is failure of the limbal cell population that normally renews the corneal epithelium. When this reserve is lost, the surface becomes unstable and may develop conjunctivalisation, vascularisation, persistent defects, and scarring.
Because reduced corneal sensation removes part of the warning system and part of the healing system at the same time. Expert consensus notes that patients may have few symptoms despite progressive epithelial breakdown, ulceration, and stromal compromise.
It acts as a biologically active scaffold that supports epithelial healing while reducing inflammation, vascularisation, and surface instability in selected ocular surface disorders.
No. Serum tears are blood-derived biological preparations that contain growth factors and proteins relevant to healing, while artificial tears primarily provide lubrication and surface protection.
It is considered when inflammation control and medical therapy alone cannot restore a stable ocular surface, or when structural deficiency of mucosa, lids, limbus, tear production, or corneal protection prevents durable healing.
Suggested short-form educational topics
These topics translate well into premium patient-facing reels, short lectures, or clinician-education clips.
Why the tear film is living biology, not just moisture
A concise explanation of how tear instability affects epithelial health, optics, and comfort.
Neurotrophic keratitis: when the cornea stops feeling and stops healing
A visual explanation of corneal sensation, epithelial breakdown, and why painless disease can still be dangerous.
How chronic inflammation turns repair into damage
Show the shift from regulated healing to matrix degradation, ulceration, and scarring.
What amniotic membrane actually does on the ocular surface
Explain scaffold biology, anti-inflammatory effects, and its role in restoring epithelial closure.
Serum tears versus artificial tears
Clarify the difference between lubrication alone and blood-derived biological support.
How corneal scars affect quality of vision
Use simple optics to explain why a healed cornea may still scatter light and reduce contrast.